Radiology has never been short on tools for looking at images. What it has been short on is a way to preserve how a case was read — the sequence of decisions, the slices that mattered, the measurements that changed the impression, the moment something clicked.
That gap shows up every day in real workflows.
A radiologist opens a study, scrolls through hundreds of slices, adjusts contrast, compares planes, draws a measurement, flags an area of concern, and forms an opinion — often while thinking out loud, dictating fragments, or keeping mental notes. Then the reading ends, and a second job begins: reconstructing that journey into a clear, structured report with the right images attached.
It is repetitive. It is easy to lose context. And it pulls attention away from the part of the work that actually requires clinical judgment.
At PYCAD, this is exactly the kind of gap we think modern imaging software should close. It sits at the intersection of the viewer experience, custom DICOM viewer development, and broader radiology AI workflow automation.
The problem is not viewing. It is remembering.
Most imaging platforms are excellent at display. They are less effective at capturing the story of a read.
Where did the radiologist look first? Which finding triggered a deeper review? Which measurement supported the final conclusion? Which view best illustrates what needs to go into the report?
That information usually lives outside the viewer — in memory, in scattered notes, in a separate dictation system, or in screenshots saved manually. The report becomes a reconstruction exercise rather than a natural continuation of the read.
For busy teams, that friction adds up. For teaching and quality review, it makes it harder to understand not just what was concluded, but why. For anyone exploring smarter clinical workflows, it leaves a large amount of valuable context on the table.
What if the read itself became the source material?
We set out to explore a simpler idea: what if you could read a case the way you already do — naturally, at your own pace — and have that session become the foundation of the report?
Not a live assistant interrupting your train of thought. Not another window to manage while you work. Just the viewer, your voice, and your normal review habits.
Start a session. Scroll. Adjust. Measure. Annotate. Speak your findings as you go — the way many radiologists already do in practice, even if informally.
When the session ends, the system brings it together: your narration, the key moments from the review, the images that matter, and a structured draft report you can refine rather than build from scratch.
Read once. Report drafted. Minutes instead of hours.
That is the experience we wanted to demonstrate.
A workflow built around how radiologists actually work
The goal was never to replace clinical judgment. It was to reduce the administrative distance between reading and reporting.
In practice, that means supporting the full rhythm of a case review:
- Moving through the study in the views that matter
- Adjusting presentation to evaluate subtle findings
- Capturing measurements and annotations where they support the impression
- Narrating observations, differentials, and recommendations in real time
- Ending with a report that reflects both the findings and the reasoning behind them
The value is not just speed. It is coherence. The report stays aligned with the read because it is derived from the read.
For the radiologist, that means less re-entry of information already formed during the case. For the team, it means reports that are easier to review, easier to teach from, and easier to trust because they carry the visual evidence alongside the text.
This also connects naturally to broader platform work around cloud DICOM platforms, custom PACS viewer development, and deployment-ready medical imaging AI software.
Why this matters beyond convenience
This kind of workflow points to something larger than a feature demo.
Medical imaging is moving toward environments where AI, automation, and advanced visualization are everywhere — but clinical adoption still depends on whether new capabilities fit naturally into existing habits.
Tools that ask clinicians to change how they think usually fail. Tools that quietly support how they already work have a much better chance.
A session-based approach respects that principle. The radiologist remains in control. The reading stays human-led. The output is assistive, not authoritative.
That matters for trust. It matters for adoption. And it matters for the future of imaging platforms that want to be more than viewers — platforms that understand clinical workflow as deeply as they understand pixels.
Why now
What makes this moment different is that the underlying pieces are finally catching up to the workflow need.
Multimodal AI can now work across voice, images, annotations, and structured outputs in the same session. Viewers can capture richer interaction context. And clinical teams increasingly expect reporting systems to be faster, more traceable, and easier to review.
The opportunity is not just to automate reporting, but to connect it more faithfully to the act of interpretation itself. Organizations like the Radiological Society of North America (RSNA) and the American College of Radiology (ACR) continue to shape the broader conversation around radiology workflow, reporting quality, and responsible clinical adoption.
What we showed in the demo
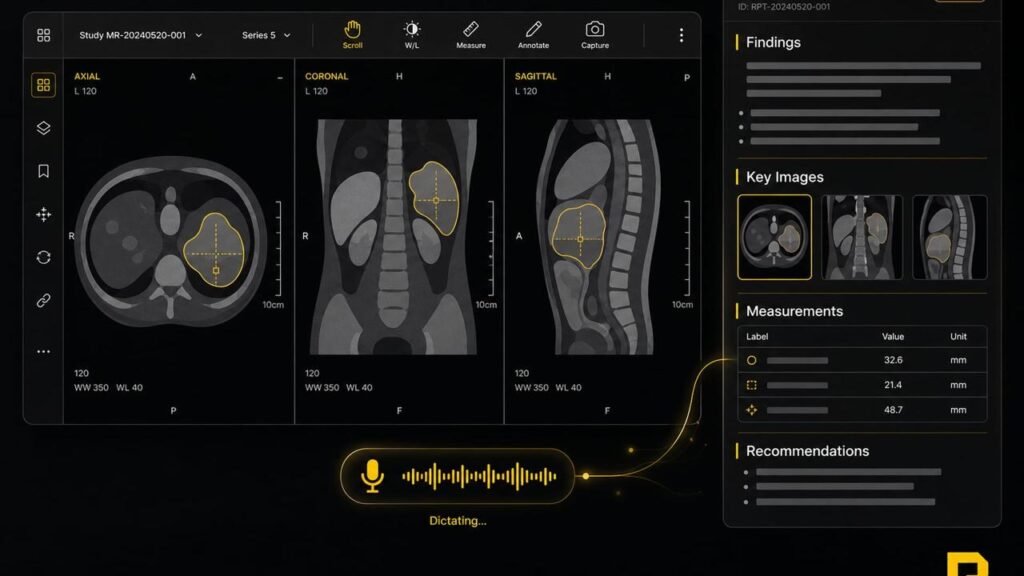
In our demonstration, we walked through a complex whole-body case with extensive segmentation and multi-planar review — the kind of study where context, sequence, and visual support all matter.
Multi-planar review in context
The session moved across axial, coronal, and sagittal views so the case could be evaluated the way radiologists actually work in practice, not through a fixed sequence imposed by software.
Segmentations and measurements tied to findings
We reviewed segmented structures and captured measurements directly where they mattered, creating a clearer connection between the visual evidence and the reasoning behind the impression.
Spoken impressions during the read
Instead of treating dictation as a separate downstream step, the workflow allows spoken findings and recommendations to become part of the same interpretive session.
Generated report with supporting images
The output combined narrative findings with the images and measurements that supported them, so the report draft reflected both the conclusion and the path taken to reach it.
The point of the demo was not to claim perfection. It was to show what becomes possible when the read and the report share the same foundation.
When that connection exists, reporting stops feeling like documentation and starts feeling like the natural end of the clinical conversation you were already having with the case.
For teams comparing approaches, this complements work we have already explored around radiology AI agents inside real DICOM workflows and the rise of CT-native foundation models for radiology AI.
More than speed: traceability and trust
A session-based workflow can also improve traceability.
Instead of a report appearing as a final text artifact disconnected from the reading process, key findings can remain linked to the measurements, views, and verbal observations that supported them. That kind of provenance can be valuable for review, collaboration, and quality assurance.
Just as importantly, the point is not to replace the radiologist’s report with an opaque automated output. It is to capture the interpretive session in a way that makes drafting faster, preserves context, and keeps the clinician firmly in charge of what is ultimately signed.
Early days, real direction
This work is still exploratory. We are testing a use case, learning from it, and refining the experience based on what clinicians actually need — not what presents well on a product roadmap.
There is a long path from a compelling demo to a routine part of daily practice. Validation, workflow integration, governance, and clinical review all matter. We take that seriously.
For this kind of workflow to matter in practice, it also has to fit into the systems around the radiologist — reporting infrastructure, image archives, review workflows, and governance requirements. The goal is not a disconnected demo experience, but a path toward integration with the environments clinicians already rely on.
If you are evaluating where this fits inside a broader product roadmap, our services and case studies pages provide more context on the kinds of imaging products and clinical tools we help build.
FAQ
How does AI-assisted radiology reporting work?
AI-assisted radiology reporting works by capturing parts of the reading session — such as measurements, annotations, selected views, and spoken findings — and using them to assemble a structured draft report. The radiologist remains responsible for review, correction, and final sign-off.
Does this replace the radiologist’s report?
No. The goal is not to replace the radiologist’s judgment or final report. The goal is to reduce repetitive documentation work and preserve the reasoning context created during the read.
Can this integrate with existing PACS and reporting systems?
That is the direction that matters most in practice. A useful workflow has to fit existing reporting infrastructure, image archives, governance requirements, and viewer environments rather than forcing clinicians into an isolated tool.
Why is a session-based radiology reporting workflow useful?
A session-based radiology reporting workflow helps keep findings, measurements, images, and spoken impressions connected. That can improve speed, traceability, teaching value, and consistency between what was reviewed and what was reported.
Disclaimer
The clinical content shown in the video is illustrative only, created to demonstrate product functionality. It does not represent a real patient case. Some medical statements in the demonstration may contain errors and should not be used for diagnostic or educational purposes without qualified clinical review. Any production use of AI-assisted reporting must remain subject to appropriate medical oversight.
The question we are really asking
Radiology does not need more ways to display images. It needs better ways to preserve clinical reasoning in the moment it happens.
If we can close the gap between reading and reporting — without adding friction, without breaking trust, without forcing a new mental model — we can give clinicians back time, improve report quality, and create a stronger foundation for the next generation of imaging workflows.
That is the problem we are interested in.
That is what this demo is about.
If you work in radiology, medical imaging, hospital informatics, or clinical AI, we would love to hear how your team handles the read-to-report gap today — where the friction shows up, what tools you use, and what would actually make a difference in daily practice.